I always loved my work as a dentist. But as time went on, my days began to feel hopeless. Day after day, I would see patients with rotten, crooked and infected teeth. I was fixing problems, but it felt like plugging holes in a boat heading for a waterfall.
Dental health was still getting worse, both among my patients and in society. I became frustrated with my practice.
Amongst tooth decay, bleeding gums and crooked teeth, I saw people with sick mouths and sick bodies. But people could rarely see the connection between the two. They just accepted dental disease as a normal part of modern life.
However, a few people WERE seeking answers. A parent would ask WHY their child’s teeth were crooked. This made me uneasy because I’d asked myself this too – and I didn’t have the answers. My training hadn’t provided them.
The turning point came when I was taking some time away from practice. By chance, I discovered Weston A Price’s Nutrition and Physical Degeneration. His words hit me like a lightning bolt. Here was a dentist that seemed to have the same concerns and questions I did. His book proclaimed to have the answers.
At first, though, I couldn’t understand his conclusions. Crooked teeth and getting braces were due to diet? How could it be true?
I was compelled by Weston A Price’s ideas. But my training was telling me to be skeptical. That conflict started me on my own journey to understand the puzzle he’d assembled. I spent the next few years trying to fill the gaps between his time and mine.
Weston A Price was describing the patients he saw as sick. I too was seeing many children with long skinny faces, open mouths and tired eyes. Their palates are narrow, high, and their teeth are cramped and crooked. These kids would grow up into adults with other chronic diseases.
Price’s message was clear. The mouth-body connection was far more important than previously thought. And an oral health diet was the core contributor to preventing braces.
An absence of the question ‘why?’
If you look through dental textbooks, you will not find a solid ‘definition’ for why so many people are getting braces.
I was certainly surprised. I’d go back to the index and chapters, sure I’d missed something. But I soon realized I hadn’t. In my training, there was very little discussion on how to prevent braces.
In my practice, I would diagnose, classify and plan treatment for crooked teeth. The same for impacted wisdom teeth as well. But I would never say why it occurred in the first place, or how it might affect the rest of the body.
The truth was I didn’t know how.
One of the big dental care problems since Weston A Price’s era is that we haven’t learned why crowded teeth happen.
A whole new world: functional dental growth
Today, the way we understand dental arch growth has exploded. Crooked teeth and impacted wisdom teeth are the endpoints of poor skeletal growth. Our teeth are the victims of the platform they live in.
When a child now walks into the dental practice, crooked teeth can be assessed in a completely new way.
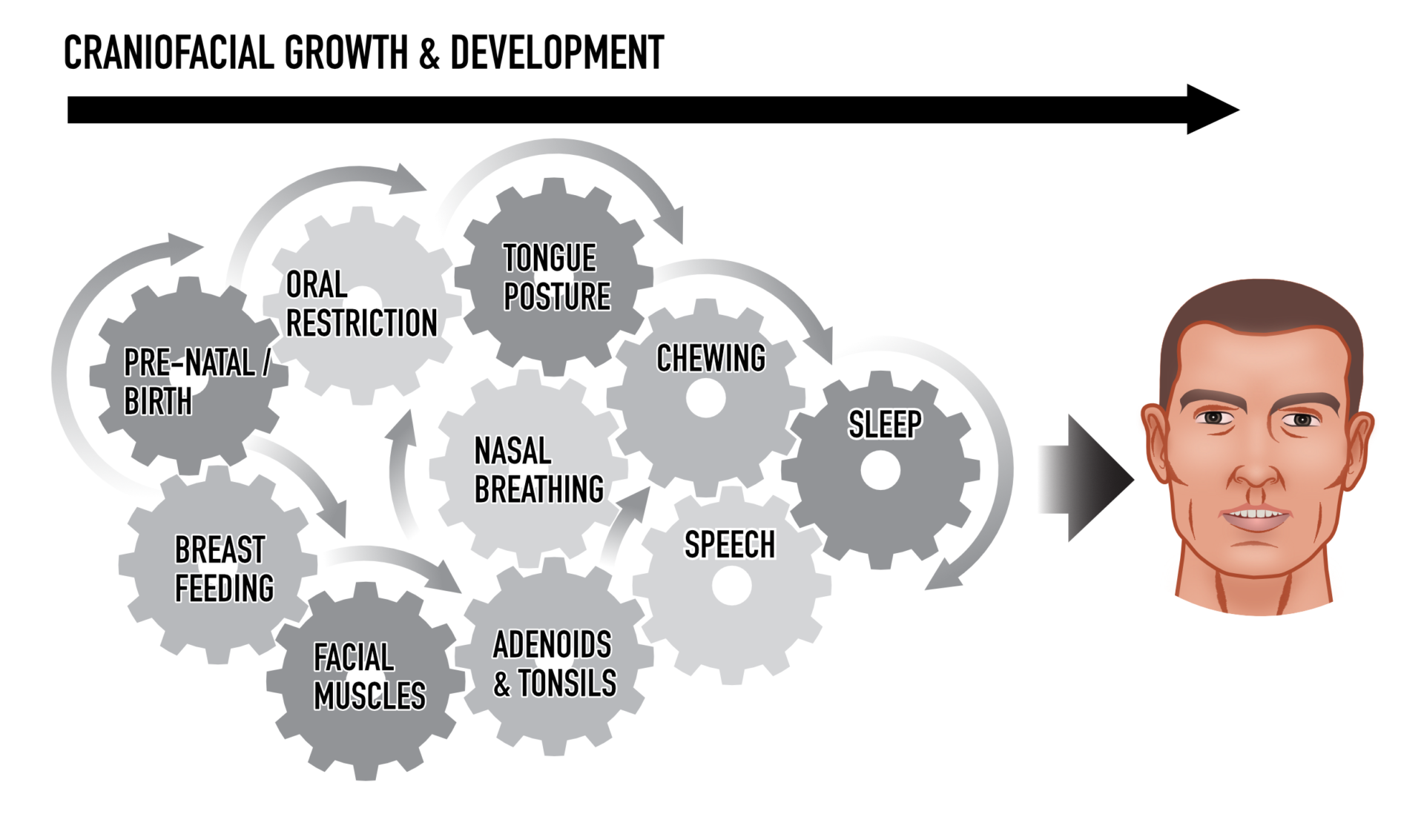
Dental growth is a function of breathing, airway and postural influences on teeth. Jaw growth is directed by feedback from the tongue, nasal airways, and facial muscles.
One way to think of this as your teeth being the ball in a football game. They’re being kicked around by the forces of the tongue, breathing and facial muscles. The dental arch isn’t passive, but a functional feedback system.
That’s why if you don’t wear a retainer after treatment with orthodontic braces, the teeth can move. This is due to an underlying functional problem.
Nasal breathing has an expansive force on the upper jaw1. Your tongue should press up against the palate, which forms the floor of the nasal airways. These forces, with closed lip muscle posture, influence whether kids avoid or prevent braces.
Why every moment matters in kid’s dental growth
Let’s go right back to the start of the problem and really understand how crooked teeth happen.
Breastfeeding is a major influence on jaw growth. It also trains a child in nasal breathing. Their tongue extracts milk by pushing the nipple to the roof of the mouth. These forces expand their palate. Breastfeeding has been shown to decrease the risk of crooked teeth2. It’s the start of a lifetime of factors that influence jaw size.
Your child’s ability to breastfeed may be due to their oral development. Ideally, the first dental exam should occur right after birth. This reveals oral restrictions, such as tongue or lip ties, which could hinder their ability to push their tongue up against the palate3. Dentists, surgeons, and ENTs can now diagnose and release tongue-ties to assist breastfeeding.
Your child continues to develop their oral muscles, lip closure, tongue posture (sitting against the palate) and breathing all influence their growth.
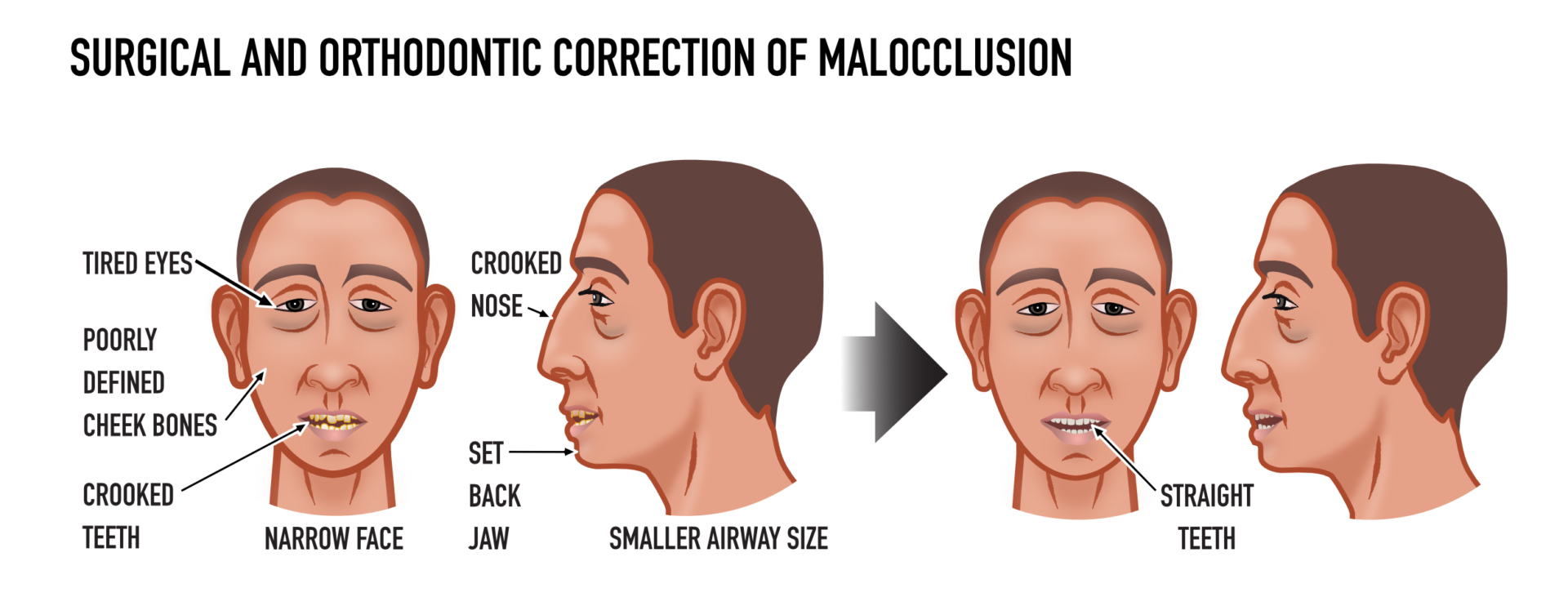
The standard orthodontic approach has been to delay action until the adult dentition has formed. In some cases, teeth are extracted and the remaining teeth straightened with braces to fit into small jaws. But this approach fails to address what caused the problem in the first place.
And our small jaws prevent us from breathing properly. Rates of sleep disorders have been increasing in the last two decades4. Without the frame to support airways when muscles relax at night, we are starving our brains of oxygen.
The end stage is obstructive sleep apnea that is linked to high blood pressure, heart failure5, and brain disease6. But upper airway resistance is a less recognized and diagnosed breathing disorder7. It’s also a driver of digestive disorders, anxiety, poor circulation and a host of other symptoms8.
Our airways aren’t only stuck in small jaw-bones, they also have swollen soft tissues. In many people, especially children, airways are also inflamed, swollen and clogged with mucus. Allergic rhinitis, asthma, swollen adenoids, and tonsils are barriers to nasal breathing9.
The oral and gut microbiome play a crucial role in how bacteria mediate the immune response. Since 2008, the scientific world has been sequencing this foreign yet symbiotic ‘organ’ that lives in the body. Imbalanced microbes cause intestinal barrier dysfunction, which is linked to digestive, autoimmune and metabolic disorders10.
The umbrella of crooked teeth has far-reaching health problems. Expansive airway focused children orthodontics can guide jaw growth11. This not only straightens teeth but considers facial and airway development.
Childhood dental development can now be guided by a team, right from birth. This includes lactation consultants, dentists, myofunctional therapists, airway orthodontics, sleep physicians, and ENTs. Functional oral health has helped us see crooked teeth are NOT inevitable.
“Crooked teeth are a solution for a complex system to remain in homeostasis. Even when some of its components are imbalanced. When you’re building a house, you start by building the foundation, then the roof, and so on. The last thing you work on is the interior – which is the teeth.”
– Dr Dave Singh
Searching for the ‘yolk’ of crooked teeth
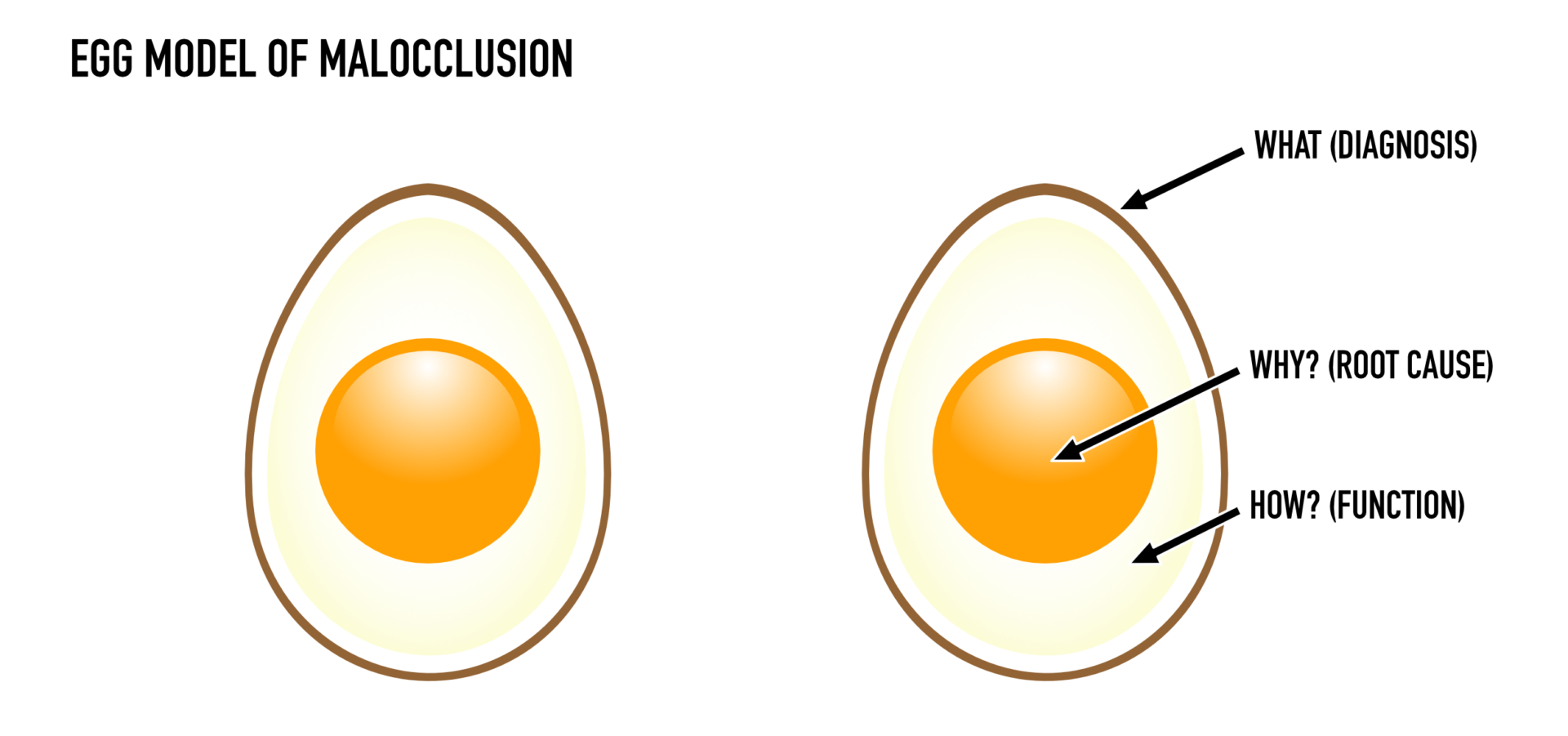
Why are so many getting braces?
The fluid model of the jaw and facial growth digs deeper into how crooked teeth occur.
But it doesn’t answer why or how to prevent braces.
This is where Weston A Price was well ahead of his time. He had found the why. Now we need to connect his theory to what science has since revealed.
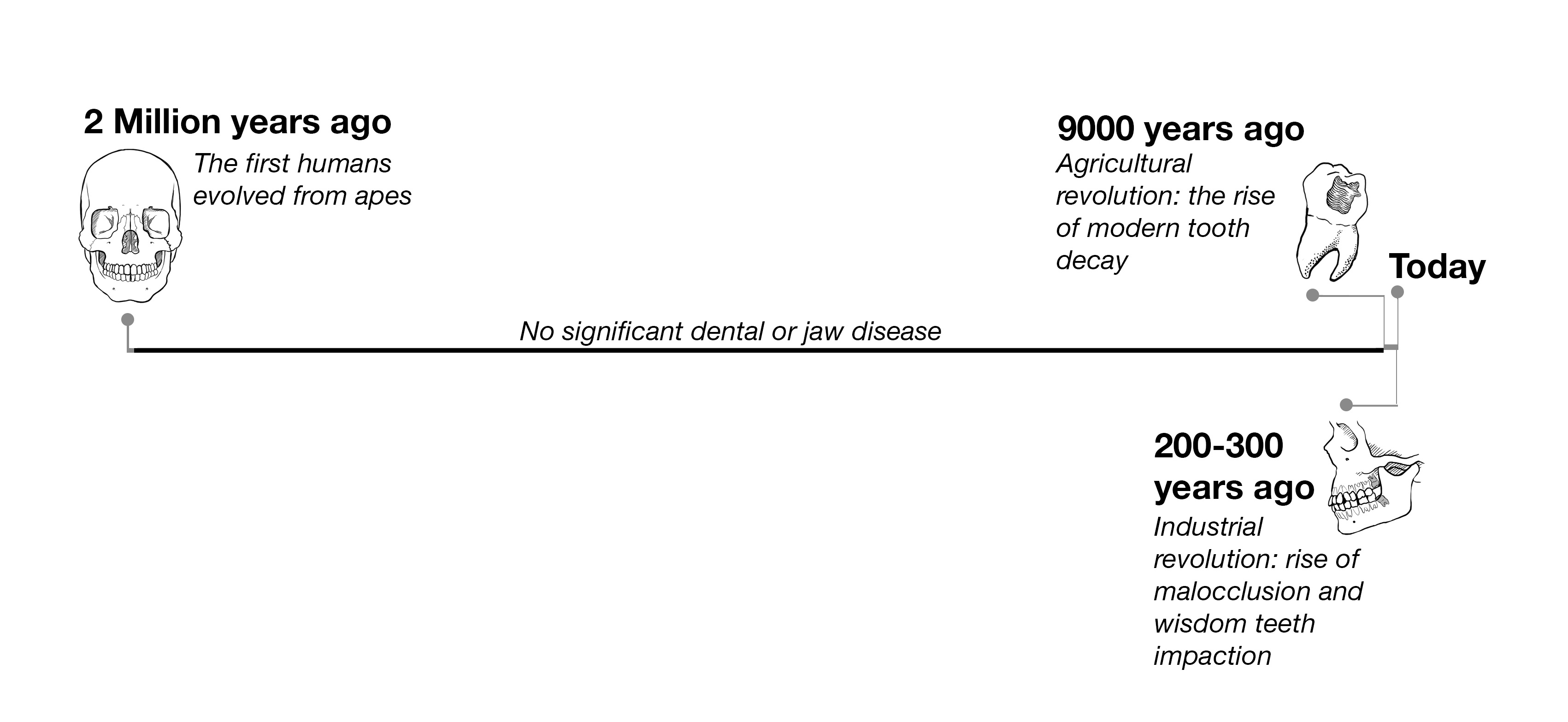
Anthropologists, such as Robert Corruccini have long confirmed that malocclusion is linked directly to historical changes to the human diet12. The human fossil simply lacks crooked teeth before farming and industry.
The history of dental disease in humans
An evolutionary, ancestral perspective is an important missing piece of the puzzle. It also helps us to dig past the ‘egg white’ layer.
Dr Kevin Boyd has proposed that neonatal jaws are failing to develop in the womb13. During growth in the womb, the fetus goes through 3D skull growth14.
Pregnant women have a higher risk of sleep apnea16 and a mother with crooked teeth may deliver less oxygen to her child. We know the relationship between low oxygen and fetal growth. This could be similar to smoking during pregnancy, which curbs the growth of the fetus15.
Mothers with small jaws may have kids with small jaws. But why didn’t the jaw grow in the first place?
Nutrition as the driving factor for jaw growth
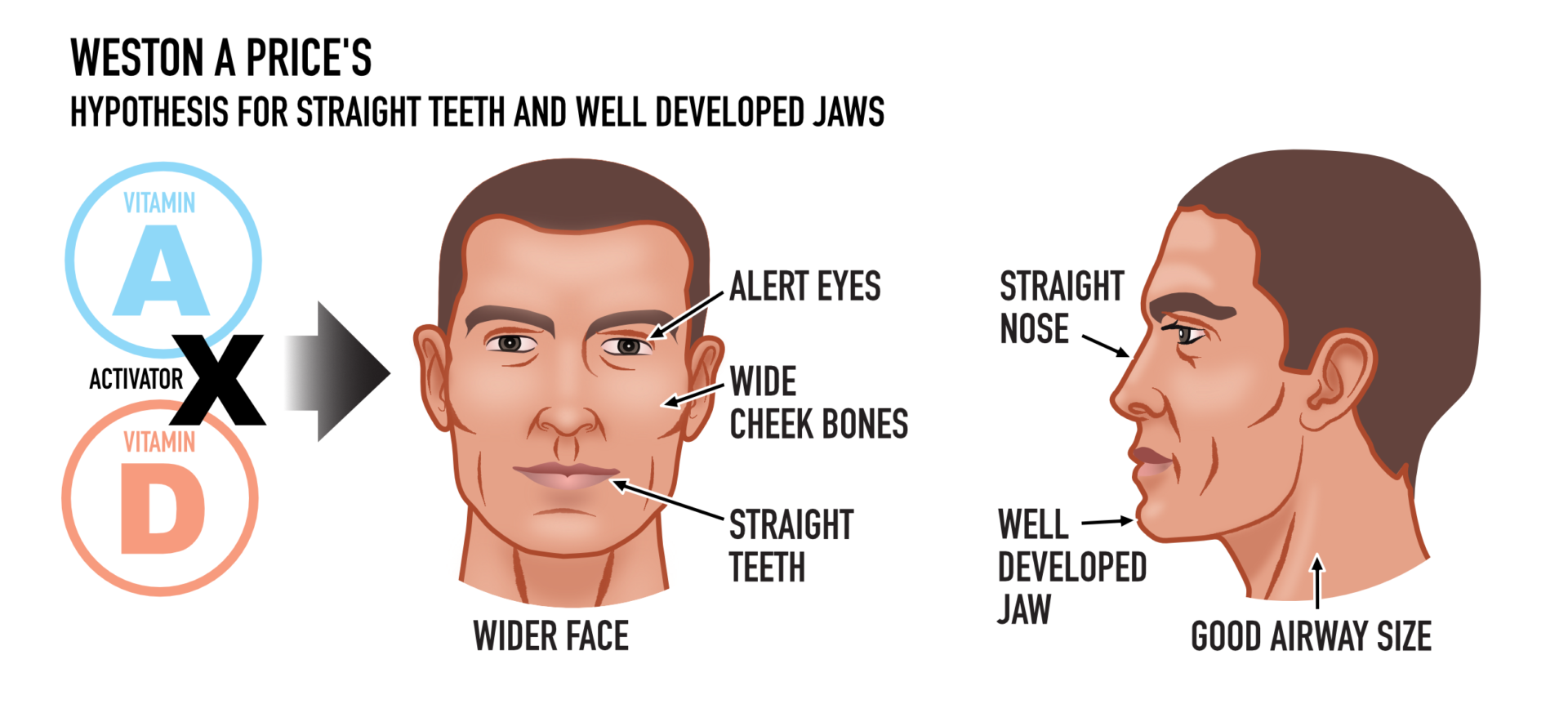
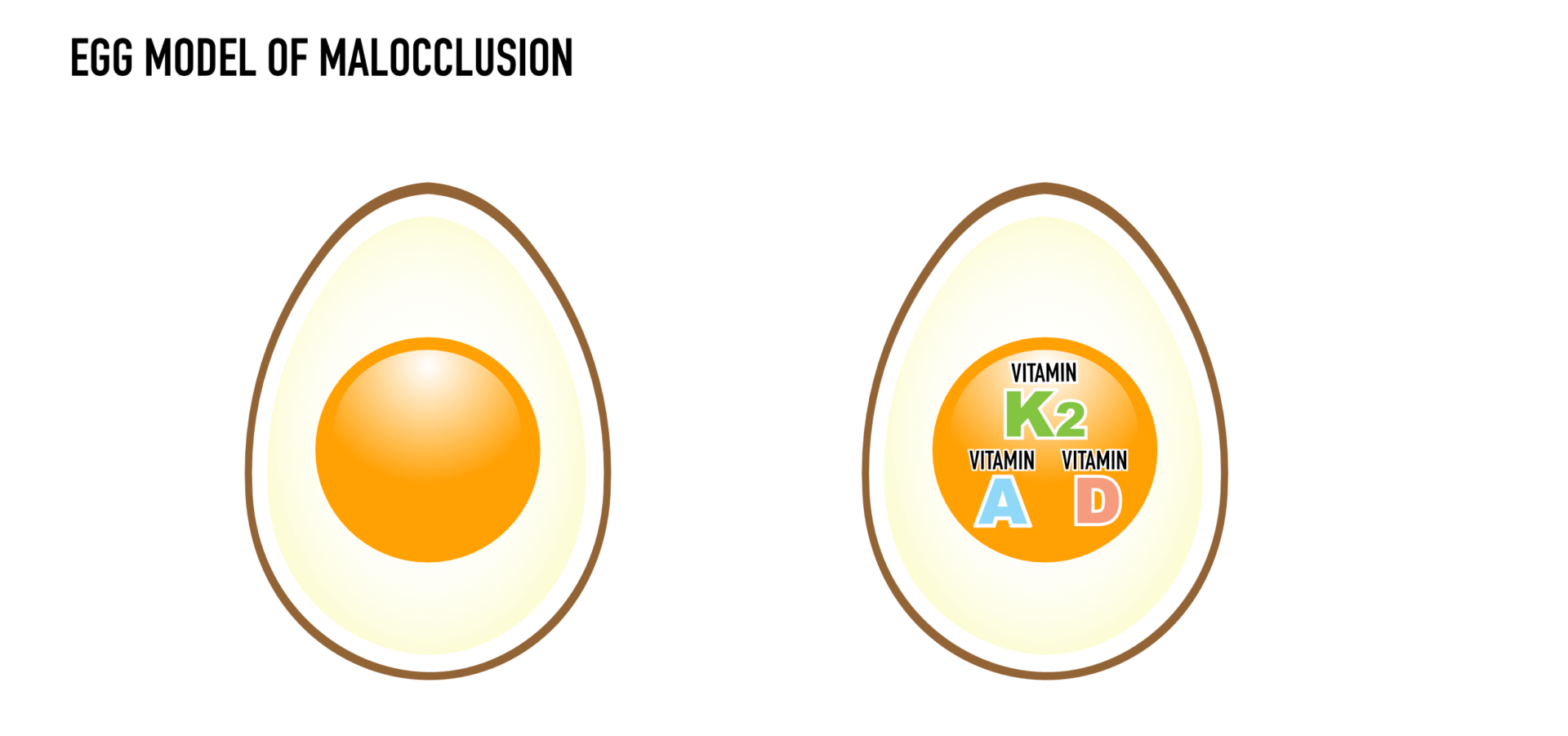
Malocclusion is linked to a major change in our food supply (lack of an oral health diet). The cranial and jaw development problems I see are linked to our diet. Weston A Price had figured this out; his theory is our ‘yolk’.
Throughout human history, a typical diet delivered foods rich in the fat-soluble vitamins D, vitamin A & vitamin K2. Today, these vitamins are sadly lacking from the modern diet. Vitamin D deficiency has been dubbed a global pandemic17.
Weston A Price’s work inspired me to begin testing all my patients with tooth decay, gum disease and malocclusion. All were insufficient, many had vitamin d deficiency.
He also noted the importance of pre-pregnancy nutrition. Vitamin D intake starts in utero and the mother carries on passing her Vitamin D to her child if she breastfeeds18. In children, low vitamin D levels have been related to tooth decay19 and adequate vitamin D may be linked to lower rates of decay20. A small amount of research has shown supplementation may prevent caries.
Bone growth is being directed by a child’s stores of vitamin D. Vitamin D deficiency in children is known to cause growth retardation21.
Vitamin D also directs cellular growth, binding to and influencing thousands of genes22. And perhaps critically, deficiency in Vitamin D directs the epigenome23.
For a long time, Weston A Price’s fat-soluble vitamins theory lacked a physiology model to support it.
However, with the help of many arms of science, we now understand crooked teeth as a food driven outcome.
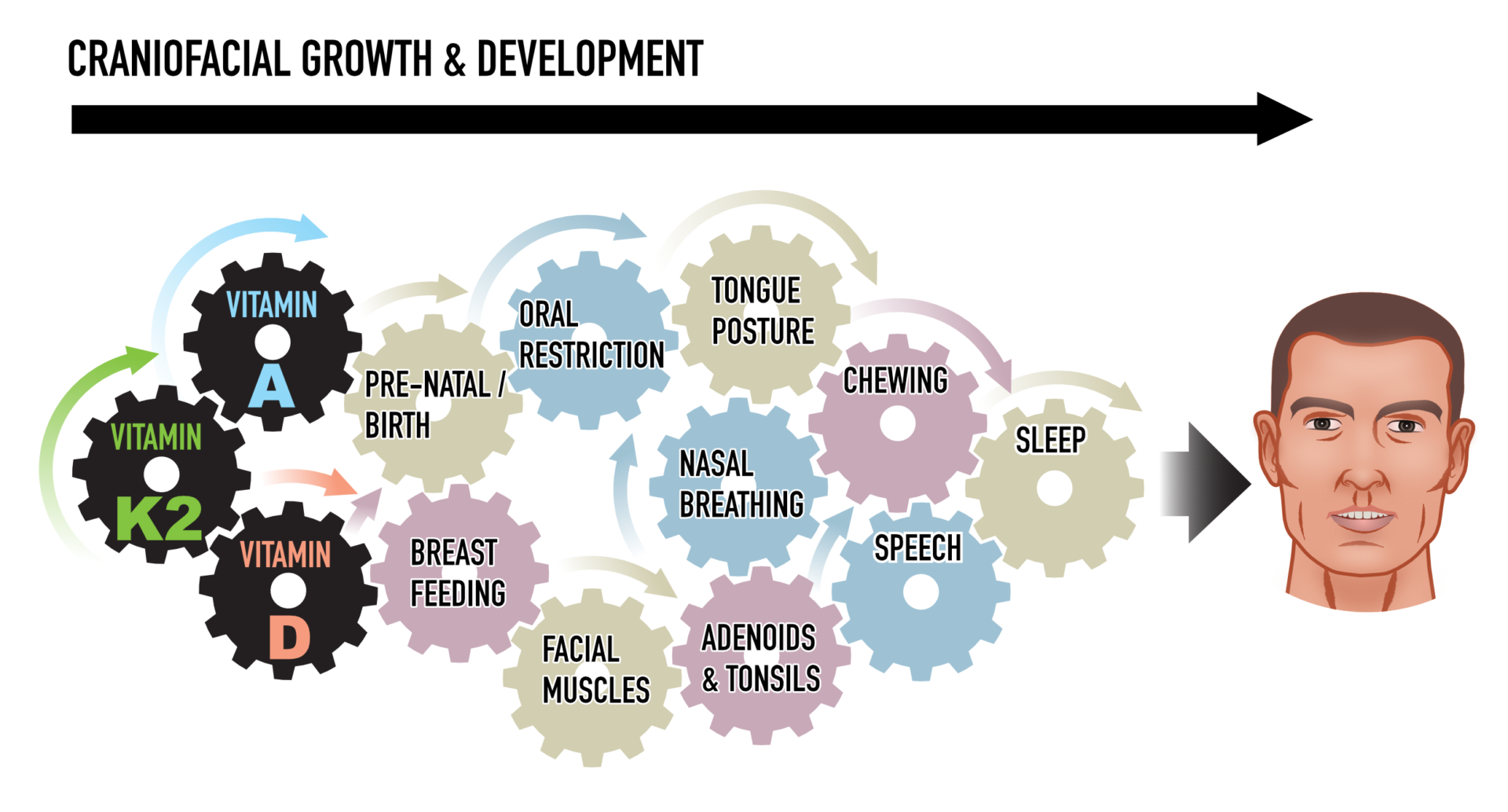
The traffic lights of growth and development
To better understand crooked teeth, let’s look at how the human body develops right from birth.
As the fetus grows, it develops different systems such as spinal cord, skeletal system and organs in an established order, with progress checkpoints. However, if one part of the body hasn’t finished, it can’t afford to wait; the show must go on.
For instance, spina bifida is due to failure to close the neural tube. These checkpoints occur around the 23rd and 27th days of pregnancy24. With adequate folate, a building block of the nervous system, the body completes its work correctly and moves onto other systems. Without enough folate, the job is left incomplete, and the child with an exposed spinal cord.
As the craniofacial system develops, it too has a series of progress checkpoints. When a child reaches a certain stage, whether inputs have been sufficient or not, the growth stages move on. A small or narrow dental arch has been left ‘unfinished’ like a spinal cord in spina bifida.
The fat-soluble vitamins and dental health – the ‘bricks and mortar of teeth’
Why the fat-soluble vitamins prevent braces
Weston A Price’s theory centered around the trilogy of fat soluble vitamins. Vitamin K2 wasn’t identified as activator X until 2007 by Chris Masterjohn. Masterjohn has since fleshed out much of their three-way synergy in the body.
Now we have reached the final pieces of the puzzle.
Let’s look at the ways that these vitamins work together to direct bone and teeth growth.
Vitamin D
Vitamin D deficiency and its impact on the skeletal system is firmly established. Osteoporosis and rickets in children (which occurs when bones don’t mineralize properly) are well known. Vitamin D is the main conductor of minerals in the body and vital for calcium absorption Vitamin D is also linked to tooth decay and gum disease.
90% of the population now have impacted wisdom teeth.
Jaw growth, like any other bone growth, is three-dimensional. In order to erupt, teeth rely on overall space in the jaw – length, but also the width of the bone25.
To gain width, the bone must go through ‘appositional’ growth. This builds the thickness of the bone and that happens in late stage development of the jaw and houses the wisdom teeth26.
Today, many children’s bodies seem to lack both the raw materials and the signals to keep this growth process growing. The jaw bones are less developed in all dimensions and wisdom teeth simply don’t ‘fit’.
Vitamin A
While bones are growing, they must remain functional. Growing bones must also support joint movements. Bone growth is a material-hungry remodeling process that must break up active bone before adding new layers.
Price established the absence of foods rich in vitamin A in the modern diet. Vitamin A activates osteoclasts that disrupt these bony surfaces to stimulate growth27.
Vitamin A also influences gene regulation, vision, reproduction, cell division and cell differentiation, and works with vitamin D throughout the body28.
Vitamin K2
While vitamin D controls calcium absorption, vitamin A supplies the workers that keep the process running. Together, they activate the proteins that stimulate demand for vitamin K229.
Like vitamins D and A, vitamin K2 is passed on to a child by their mother30. Vitamin K2 deficiency is likely far more prevalent than it is currently acknowledged. It activates the protein osteocalcin that carries minerals into bones. Once osteocalcin is activated by K2, its receptors for calcium ‘open’ and allow it to carry minerals into bone and teeth31. It works with vitamin D in osteoblasts to produce bone32.
Another protein activated by Vitamin K2 is MGP protein. MGP protein has the task of stopping minerals going into the soft tissues, including vascular tissues33.
Rats show that septal calcification may cause deviated septum which may prevent the functional growth of the maxilla by reducing nasal breathing34. However, studies need to confirm this relationship35.
All three fat-soluble vitamins are the heart of our yolk – Weston A Price’s theory.
The nutritional model of malocclusion – the real oral health diet
Food is the primary cause of crooked teeth and why so many kids today are getting braces. An oral health diet should be our primary concern when creating dietary guidelines.
Many factors combine to influence jaw and teeth growth, and many nutrients combine to influence the body and its development. To date, nutrition research has focused on the action of one vitamin and one outcome. However, the fat-soluble vitamins work together in a system.
A reductionist approach that studies how nutrients work in isolation fails to account for the complexity of human growth and development.
Weston A Price taught us to look at the body and the mouth as a whole system. Today, with the benefit of ancestral medicine, the human microbiome and epigenetics, we can progress forward with a complete explanation for his theory.
Now we want to hear from you. Please leave your questions in the comments below.
For more information on Dr. Lin’s clinical protocol that highlights the steps parents can take to prevent dental problems in their children: Click here.
Want to know more? Dr Steven Lin’s book, The Dental Diet, is available to order today. An exploration of ancestral medicine, the human microbiome and epigenetics it’s a complete guide to the mouth-body connection. Take the journey and the 40-day delicious food program for life-changing oral and whole health.
Click below to order your copy now:
US AMAZON
US Barnes & Noble
UK AMAZON
Australia BOOKTOPIA
Canada INDIGO
References:
- Gungor, Ahmet Yalcin, and Hakan Turkkahraman. “Effects of airway problems on maxillary growth: a review.” Eur J Dent 3.3 (2009): 250-4.
- Peres, Karen Glazer, et al. “Effect of breastfeeding on malocclusions: a systematic review and meta‐analysis.” Acta Paediatrica 104.S467 (2015): 54-61.
- Rowan-Legg, Anne. “L’ankyloglossie et l’allaitement.” Paediatrics & child health 20.4 (2015): 214.
- Peppard, Paul E., et al. “Increased prevalence of sleep-disordered breathing in adults.” American journal of epidemiology 177.9 (2013): 1006-1014.
- Jean-Louis, Girardin, et al. “Obstructive sleep apnea and cardiovascular disease: role of the metabolic syndrome and its components.” J Clin Sleep Med 4.3 (2008): 261-72.
- Pan, Weihong, and Abba J. Kastin. “Can sleep apnea cause Alzheimer’s disease?.” Neuroscience & Biobehavioral Reviews 47 (2014): 656-669.
- Exar, Elliott N., and Nancy A. Collop. “The upper airway resistance syndrome.” CHEST Journal 115.4 (1999): 1127-1139.
- Pepin, J. L., et al. “The upper airway resistance syndrome.” Respiration 83.6 (2012): 559-566.
- Small, Peter, and Harold Kim. “Allergic rhinitis.” Allergy, Asthma & Clinical Immunology 7.1 (2011): S3.
- Ursell, Luke K., et al. “Defining the human microbiome.” Nutrition reviews 70.suppl 1 (2012): S38-S44.
- Aziz, Tehnia, et al. “Effect of non-surgical maxillary expansion on the nasal septum deviation: a systematic review.” Progress in orthodontics 16.1 (2015): 1-7.
- Ciochon, Robert L., R. A. Nisbett, and R. S. Corruccini. “Dietary consistency and craniofacial development related to masticatory function in minipigs.” Journal of craniofacial genetics and developmental biology 17.2 (1996): 96-102.
- Herlin, Christian, et al. “Modeling of the human fetal skull base growth: interest in new volumetrics morphometric tools.” Early human development 87.4 (2011): 239-245.
- Holder-Espinasse M, Abadie V, Cormier-Daire V. et al. Pierre Robin sequence: a series of 117 consecutive cases. J Pediatr. 2001;139(4):588–590.
- Delpisheh, Ali, et al. “Prenatal smoking exposure and asymmetric fetal growth restriction.” Annals of human biology 35.6 (2008): 573-583.
- Sahota, Pradeep K., Sanjay S. Jain, and Rajiv Dhand. “Sleep disorders in pregnancy.” Current opinion in pulmonary medicine 9.6 (2003): 477-483.
- Holick, Michael F., and Tai C. Chen. “Vitamin D deficiency: a worldwide problem with health consequences.” The American journal of clinical nutrition 87.4 (2008): 1080S-1086S.
- Hollis, Bruce W., et al. “Maternal versus infant vitamin D supplementation during lactation: a randomized controlled trial.” Pediatrics 136.4 (2015): 625-634.
- Hujoel, Philippe P. “Vitamin D and dental caries in controlled clinical trials: systematic review and meta-analysis.” Nutrition reviews 71.2 (2013): 88-97.
- University of Washington. “Vitamin D linked to lower rates of tooth decay.” ScienceDaily. ScienceDaily, 27 November 2012. <www.sciencedaily.com/releases/2012/11/121127130321.htm>.
- Holick, Michael F. “Resurrection of vitamin D deficiency and rickets.” The Journal of clinical investigation 116.8 (2006): 2062-2072.
- Samuel, Sam, and Michael D. Sitrin. “Vitamin D’s role in cell proliferation and differentiation.” Nutrition reviews 66.suppl 2 (2008): S116-S124.
- Fetahu, Irfete S., Julia Höbaus, and Eniko Kállay. “Vitamin D and the epigenome.” Genome-wide view on the physiology of vitamin D (2014): 61.
- Pitkin, Roy M. “Folate and neural tube defects.” The American journal of clinical nutrition 85.1 (2007): 285S-288S.
- Kaur, Rachninder, et al. “Early prediction of mandibular third molar eruption/impaction using linear and angular measurements on digital panoramic radiography: A radiographic study.” Indian Journal of Dentistry 7.2 (2016): 66.
- Mundy, Gregory R. “Regulation of bone formation by bone morphogenetic proteins and other growth factors.” Clinical orthopaedics and related research 324 (1996): 24-27.
- Hayes, K.C. & Cousins, R.J. Calc. Tis Res. (1970) 6: 120. doi:10.1007/BF02196191
- Gerster, Helga. “Vitamin A-functions, dietary requirements and safety in humans.” International journal for vitamin and nutrition research 67.2 (1997): 71-90.
- Patti, Aurora, et al. “Endocrine actions of osteocalcin.” International journal of endocrinology 2013 (2013).
- Motohara, Kunihiko, et al. “Oral supplementation of vitamin K for pregnant women and effects on levels of plasma vitamin K and PIVKA-II in the neonate.” Journal of pediatric gastroenterology and nutrition 11.1 (1990): 32-36.
- Hauschka, P. V. “Osteocalcin: the vitamin K-dependent Ca2+-binding protein of bone matrix.” Pathophysiology of Haemostasis and Thrombosis 16.3-4 (1986): 258-272.
- Koshihara, Yasuko, and Kazuko Hoshi. “Vitamin K2 enhances osteocalcin accumulation in the extracellular matrix of human osteoblasts in vitro.” Journal of Bone and Mineral Research 12.3 (1997): 431-438.
- Theuwissen, Elke, Egbert Smit, and Cees Vermeer. “The role of vitamin K in soft-tissue calcification.” Advances in Nutrition: An International Review Journal 3.2 (2012): 166-173.
- Howe, Andrew M., and William S. Webster. “Vitamin K—its essential role in craniofacial development.” Australian dental journal 39.2 (1994): 88-92.
- D’Ascanio, Luca, et al. “Craniofacial growth in children with nasal septum deviation: a cephalometric comparative study.” International journal of pediatric otorhinolaryngology 74.10 (2010): 1180-1183.




17 Responses
I’m so happy that all the farm fredh eggs we eat are part of the solution.
Hi Bee,
Thank you for the tip! WE love Eggs too 😉
Great article but not sure why you only talk about braces and how the face looks… Many parents still view that as a ‘nice to have’… whereas this stuff goes a million times deeper into being:
1) the root cause of almost all postural problems
2) the root cause of probably almost all neurological issues
3) the root cause of most heart disease and some cancers
4) the root cause behind most obesity
5) the root cause behind probably 70%+ of deaths
The public needs to be aware of just how deep this goes…
Hi Ken,
Yes completely agree here. As you say these problems reverberate right throughout the body. The skeletal system is connected after all?
Steven
A very interesting article! As someone currently with braces I can see how I ended up with crooked teeth, as a mother I find this information so helpful as my boys grow.
Hi Amy,
Yes! It’s really important to realize right from an early age. Every meal and even breathe is influencing how your kid’s teeth are developing
Great article Dr Lin! This information really resonates with me. At the age of 12, I had 4 teeth removed, followed by braces for two years to correct overcrowding. All seemed to be fine when I had my braces removed at age 14 but slowly my teeth became crooked again and I had 4 horizontally impacted wisdom teeth removed at the age of 19. I am now in my 30’s and I suffer from bruxism and jaw pain. Back pain that started when I was 10 years of age has worsened with age. My teeth are also starting to go crooked again. I didn’t wear a retainer so this does make sense in hindsight. I have been told by my current dentist that my teeth should never have been removed but that bone should have been grown to make space for my teeth. I have read that crooked teeth / crowding are often a result of incorrect oral posture and/or mineral deficiencies. It just so happens that I am very low in vitamin D and probably have been for some time. My diet as a child and teen was also quite poor. Your article is very enlightening. Thank you for the research that you do and for writing articles like this for the general public! We need doctors like you who tell it like it is! I see a brighter future for overall health and dentistry.
Hi Connie, thanks so much and sorry to hear about the problems you’ve experienced. These processes that result in stop our jaws from growing also continue throughout life, so important to get everything on track moving forward!
What can we as adults do now if we have had this kind of history (poor diet growing up, problems with teeth and gums etc). Do you have info/articles/suggestions on that? Thank you! 🙂
Hi, Yes there are options for adult expansive therapy. It aims to correct jaw growth and widen airways. There will be info up on the website here shortly!
Fantastic article-thank you! This explains a lot 🙂
Thanks Rene, glad you enjoyed it!
Thanks for a great article. I’ve been following the Weston A Price principles for many years now. Four of our five grown kids have beautiful straight teeth (never had braces) & none had their wisdom teeth removed.
I don’t believe we came from apes..absolutely no proof of it. And lies have certainly but exposed on this theory.
An amazing connection you’ve made here Steve.
“Pregnant women have a higher risk of sleep apnea16 and a mother with crooked teeth may deliver less oxygen to her child. We know the relationship between low oxygen and fetal growth. This could be similar to smoking during pregnancy, which curbs the growth of the fetus15.
Mothers with small jaws may have kids with small jaws. But why didn’t the jaw grow in the first place?
Came here from Revolution Health Radio, very interesting and revelatory information. Thank you for your research!
Thank you Dr. Lin.
This goes very deep and we all are victims of looking at dental problems only through the more or less sugar in the diet and orthodentics.
Hi Aviva,
Thanks for your support. Hope this helps!
Chelsea
Community Manager
http://www.drstevenlin.com